Therapeutic value of zinc supplementation in acute and persistent diarrhea: a systematic review.
Study Design
- Тип исследования
- Meta-Analysis
- Популяция
- children
- Вмешательство
- Therapeutic value of zinc supplementation in acute and persistent diarrhea: a systematic review. None
- Препарат сравнения
- None
- Первичный исход
- diarrhea
- Направление эффекта
- Mixed
- Риск систематической ошибки
- Low
Abstract
BACKGROUND: For over a decade, the importance of zinc in the treatment of acute and persistent diarrhea has been recognized. In spite of recently published reviews, there remain several unanswered questions about the role of zinc supplementation in childhood diarrhea in the developing countries. Our study aimed to assess the therapeutic benefits of zinc supplementation in the treatment of acute or persistent diarrhea in children, and to examine the causes of any heterogeneity of response to zinc supplementation. METHODS AND FINDINGS: EMBASE, MEDLINE and CINAHL databases were searched for published reviews and meta-analyses on the use of zinc supplementation for the prevention and treatment of childhood diarrhea. Additional RCTs published following the meta-analyses were also sought. The reviews and published RCTs were qualitatively mapped followed by updated random-effects meta-analyses, subgroup meta-analyses and meta-regression to quantify and characterize the role of zinc supplementation with diarrhea-related outcomes. We found that although there was evidence to support the use of zinc to treat diarrhea in children, there was significant unexplained heterogeneity across the studies for the effect of zinc supplementation in reducing important diarrhea outcomes. Zinc supplementation reduced the mean duration of diarrhea by 19.7% but had no effect on stool frequency or stool output, and increased the risk of vomiting. Our subgroup meta-analyses and meta-regression showed that age, stunting, breast-feeding and baseline zinc levels could not explain the heterogeneity associated with differential reduction in the mean diarrheal duration. However, the baseline zinc levels may not be representative of the existing zinc deficiency state. CONCLUSIONS: Understanding the predictors of zinc efficacy including the role of diarrheal disease etiology on the response to zinc would help to identify the populations most likely to benefit from supplementation. To improve the programmatic use of zinc, further evaluations of the zinc salts used, the dose, the frequency and duration of supplementation, and its acceptability are required. The significant heterogeneity of responses to zinc suggests the need to revisit the strategy of universal zinc supplementation in the treatment children with acute diarrhea in developing countries.
Кратко
It was found that although there was evidence to support the use of zinc to treat diarrhea in children, there was significant unexplained heterogeneity across the studies for the effect of zinc supplementation in reducing important diarrhea outcomes, suggesting the need to revisit the strategy of universal zinc supplementation.
Full Text
Therapeutic Value of Zinc Supplementation in Acute and Persistent Diarrhea: A Systematic Review
Archana Patel1,2., Manju Mamtani1,3., Michael J. Dibley4, Neetu Badhoniya1, Hemant Kulkarni1,3*
1 Lata Medical Research Foundation, Nagpur, India, 2Indira Gandhi Government Medical College, Nagpur, India, 3 The University of Texas Health Science Center at San Antonio, San Antonio, Texas, United States of America, 4The Sydney School of Public Health, The University of Sydney, Sydney, Australia
Introduction
Despite significant improvements in the interventions to treat diarrhea in children, it continues to pose a daunting public health challenge, especially in children from developing countries. Recent estimates suggest that nearly 3% of neonatal mortality and 17% of under-five child mortality is attributable to diarrhea. Asia and Africa have an alarmingly high incidence of childhood diarrhea. [1,2,3] Although the burden of the diarrhea-related mortality has significantly decreased since the introduction of oral rehydration therapy in 1980, diarrheal diseases in children remain a substantial global health problem. [4,5,6] In 2004, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) took two significant steps to reduce this burden by recommending the use of low-osmolarity oral rehydration solution (ORS), and supplementation with zinc for up to two weeks as part of the case management of acute diarrhea. [7,8]
The latter recommendation was based on the results of several randomized controlled trials, meta-analyses [9] and reviews [10,11,12,13] reported from around the world that have demonstrated the utility of zinc supplementation to shorten the duration of diarrhea and improve other diarrhea related outcomes. Nearly five years have elapsed and substantial additional evidence [14,15,16,17,18,19] has accumulated since the inception of the practice of zinc supplementation. The existing paradigm strongly supports the notion of zinc supplementation; however, recent scientific reports suggest several interesting cues described below indicate that a more focused approach to zinc supplementation may be required.
First, WHO/UNICEF recommends zinc supplementation for diarrhea in developing countries only. [19] The underlying justification for this is the differential prevalence of zinc deficiency. Extension of this line of thought would suggest that differential levels of zinc deficiency in individuals or populations within
developing countries might modulate the therapeutic benefits attributable to zinc. Second, five meta-analyses have been published thus far [9,16,17,18,20,21]that have all observed a protective effect of zinc on some diarrhea outcomes, but all of these meta-analyses have also reported a significant degree of heterogeneity in effect sizes across studies. Such heterogeneity raises concerns regarding the reliability of the synthetic estimates of the use of zinc supplementation. Third, evidence is emerging that zinc supplementation is not equally effective against all causative organisms. [22,23] Since the causes of acute diarrhea even within developing countries vary widely, the efficacy of zinc supplementation is likely to be heterogeneous. Lastly, it is not clear at present how zinc supplementation complements, if at all, other possible options like vitamin A supplementation and multivitamin supplementation. [23,24,25]
Together, these issues indicate the need for a closer look at the evidence that underpins the policy of blanket zinc supplementation to children with diarrhea in developing countries. This study aimed to assess the therapeutic benefits of zinc supplementation in the treatment of acute or persistent diarrhea in children, and to examine the causes of any heterogeneity of response to zinc supplementation.
Methods Data Extraction
Data extraction for this study was conducted in two steps. First, we searched the EMBASEH, CINAHLH and MEDLINEH databases for published trials on zinc supplementation. The full strategy for searching these databases and the results obtained are shown in Figure 1. Second, we collected the published reviews and meta-analyses in this field. For this, we searched the same databases using the query ‘‘zinc AND diarrhea’’ and limiting the citations to reviews, we identified 129 review articles of which 50 dealt with ‘‘zinc supplementation’’. Further restricting the articles to publication type ‘‘meta-analysis’’ identified 10 articles of which seven had formally conducted synthesis of published trials on the preventive or the therapeutic role of zinc in acute or persistent diarrhea. Five of these seven meta-analyses related to the therapeutic use of zinc in diarrhea. We carefully reviewed these five meta-analyses for any additional studies that we may have missed in the first stage of the search (Figure 1, step 7). In total, we identified 26 trials for acute diarrhea and 6 trials for persistent diarrhea. Attached at the end of the manuscript are the PRISMA statement and flowchart detailing the methods of data extraction and abstraction.
Analytical approach
We constructed a correspondence map of the published studies and meta-analyses to identify which studies were included in the different meta-analyses. We then summarized the findings from these meta-analyses into diarrhea-related clinical end-points. For each outcome, we examined the reported summary effect sizes and the heterogeneity across studies. For quantifying heterogeneity, we used the I2 statistic since it is comparable across meta-analyses. [26] If a meta-analysis reported the Q test result for heterogeneity then the I2 statistic was estimated from it using the formula I2=(Q-df)/Q with the minimum bound set to zero.
For major outcomes that showed significant summary beneficial effect of zinc on diarrhea, and which showed large heterogeneity across trials, we investigated the potential contributors to the heterogeneity. First, we conducted an updated meta-analysis to include the results from other studies that the previous metaanalyses may have omitted. For these meta-analyses, we used the
random effects model of DerSimonian and Laird. [27] Depending on the diarrhea related outcome, we used standardized mean difference or summary odds ratios as the summary measures for effect size. For diarrhea-related outcomes showing substantial heterogeneity across studies, we then estimated the contribution of potential predictors of effect size to between-study heterogeneity. For predictor variables that were categorical in nature (geographic location and setting of the study, zinc salt used, co-intervention used, and adequacy of blinding procedures) we used subgroup meta-analyses. For continuous predictor variables we conducted univariate meta-regression analyses as recommended by Higgins et al [26] and Thomson et al [28]. Continuous variables included in these analyses were: mean age, dose of zinc, duration of diarrhea before admission, proportion wasted defined as weightfor-age z score,-2, proportion stunted defined as height-for-age z score,-2, mid-arm circumference, proportion with fever, mean dehydration score, baseline zinc and proportion breastfed. Statistical analyses were conducted using the Stata 10.2 (Stata Corp, College Station, TX) software package.
Results
Systematic map of published meta-analyses on zinc supplementation in diarrhea
In 1998, Black et al [10] conducted the first focused literature review of zinc supplementation, which provided a significant
impetus for the formulation of the WHO/UNICEF recommendation [7] six years later on the use of zinc in the treatment of childhood diarrhea. Together the published meta-analyses have summarized data from 23 randomized controlled trials (9,958 children receiving zinc and 9,940 subjects receiving placebo) excluding four studies [29,30,31,32] published after the metaanalyses. For ease of identification, these meta-analyses are labeled chronologically as M1–M5 in Table 1.
The RCTs of the therapeutic effects of zinc supplementation during diarrhea have reported a wide variety of diarrhea-related outcomes. For example, these RCTs report the domain of diarrheal duration in various ways as mean duration of diarrhea since initiation of treatment, the percentage reduction in the duration of diarrhea, and the proportion of children with continued diarrhea beyond a predefined number of days (1, 3, 5 or 7). In addition, other outcomes have included stool frequency, stool output, risk of vomiting and risk of watery stools. All the five meta-analyses [9,15,16,17,18] and most of the published randomized controlled trials have however, reported the effect of zinc supplementation on mean diarrheal duration. Two meta-analyses
- Table 1. Published studies therapeutic use of zinc against in acute diarrhea.
No Author [Ref] Year Zn Pl M1 M2 M3 M4 M5
- 1 Sachdev et al [57] 1990 20 20 X X
- 2 Sazawal et al [47] 1995 456 481 X X X X X
- 3 Roy et al [45] 1997 37 37 X X X X
- 4 Hidayat et al [42] 1998 738 659 X X X X
- 5 Roy et al [53] 1998 95 95 X X
- 6 Faruque et al [39] 1999 341 340 X X X
- 7 Dutta et al [38] 2000 44 36 X X X X
- 8 Khatun et al [50] 2001 44 44 X
- 9 Strand et al [48] 2002 442 449 X X X
- 10 Bahl et al [34] 2002 806 401 X X X
- 11 Baqui et al [66] 2002 3974 4096 X
- 12 Al-Sonboli et al [33] 2003 37 37 X X X X
- 13 Polat et al [44] 2003 92 90 X X X X
- 14 Bhatnagar et al [35] 2004 132 134 X X X X
- 15 Brooks et al [37] 2005 171 89 X X X X
- 16 Larson et al [67] 2005 534 533 X X
- 17 Patel et al [43] 2005 102 98 X X
- 18 Valery et al [25] 2005 107 108 X
- 19 Fischer Walker et al [40]
- 20 Awasthi et al [49] 2006 1010 992 X
- 21 Boran et al [36] 2006 150 130 X X
- 22 Roy et al [52] 2007 28 28 X X
- 23 Gregorio et al [41] 2007 60 57 X X
- 24 Roy et al [32] 2008 82 82 X
- 25 Patel et al [31] 2009 535 273
- 26 Fijolu et al [29] 2009 30 30
X indicates that the trial was included in the specified meta-analysis. M1, Bhutta et al 2000 [9]; M2, Lukacik et al 2008 [17]; M3, Patro et al 2008 [18]; M4, Lazzerini et al 2008 [16]; M5, Haider and Bhutta [15]. Zn, Lumber of subjects in the Zn supplementation Group; Pl, Number of subjects in the placebo Group.
- doi:10.1371/journal.pone.0010386.t001
[9,17], report that there is about 15–16% reduction in the mean duration of acute diarrhea while four meta-analyses [15,16,17,18] report that zinc supplementation can reduce the acute diarrheal duration by 0.24 to 0.67 days (Table 2). Again, for this important outcome, the more recent meta-analyses [15,16,17,18] suggested that the published evidence demonstrates a statistically significant degree of heterogeneity with I2 statistic ranging from 73% to 85% (Table 2). Alternatively expressed, zinc supplementation appears to reduce the risk of continued diarrhea beyond 7 days by 29% (Table 2), although the results were heterogeneous across the published literature (I2.70%). On the other hand, zinc supplementation does not provide a statistically significant reduction in stool frequency or stool output and this evidence was not heterogeneous (Table 2).
Meta-analytical synthesis of the influence of zinc supplementation is available for three more outcomes: persistent diarrhea, vomiting after zinc administration and childhood mortality. A smaller number of trials provide the current evidence for the effects of zinc supplementation on persistent diarrhea compared to acute diarrhea. Nonetheless, zinc supplementation offers a clear benefit for persistent diarrhea and this effect was homogeneous across the published studies (Table 3). Three meta-analyses [16,17,18] have summarized the results from randomized controlled trials with vomiting as an outcome, all of which found that the risk of vomiting significantly increased after zinc supplementation [point estimates for odds ratios (OR) ranging from 1.22 to 1.71, Table 2]. The most recent meta-analysis reported significant heterogeneity across study results (I2 69%, Table 2).
Investigation into the heterogeneity: meta-analyses and meta-regressions
The systematic map shows that accompanying the influence of zinc supplementation on diarrhea was heterogeneity of the results across the published trials. We therefore conducted an investigation into the potential contributors to this heterogeneity. Summarizing results from Tables 1 and 2, we focused our analyses on two outcomes: mean duration of diarrhea in therapeutic trials and the risk of vomiting in therapeutic trials. For each of these outcomes we first implemented a random effects meta-analysis and then undertook subgroup meta-analysis and meta-regression.
Zinc supplementation and mean diarrheal duration from therapeutic trials. Our updated meta-analysis for this outcome (Figure 2) showed that the published data come off 26 comparisons from 19 trials [25,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] representing 8,957 children. We excluded trials that either studied the effects of zinc supplementation on future episodes or did not report the mean duration (and measures of variability) of the current diarrheal episodes [29,49,50,51,52,53]. Our results support a statistically significant effect of zinc supplementation on mean diarrheal duration [standardized mean difference (SMD) 20.25, 95% CI 0.35– 0.15]. Considering the statistical properties of SMD [54], this translates into a reduction in mean diarrheal duration by 19.7% (95% CI 11.9%–27.4%). The extent of heterogeneity across studies was statistically significant (I2 86.5%, p,0.001). For this outcome our subgroup meta-analyses (Table 4) showed that the country of origin could not explain the heterogeneity, however age ,12 months and study setting were associated with a differential reduction in the mean diarrheal duration. We also observed that the beneficial effect of zinc was influenced by studies that recruited all the study subjects before 12 months of age. We observed that in the five study groups from two studies that recruited infants only the SMD was 0.06 whereas when analysis was restricted to the studies that included other age groups also the SMD was 20.32 – a difference
Figures
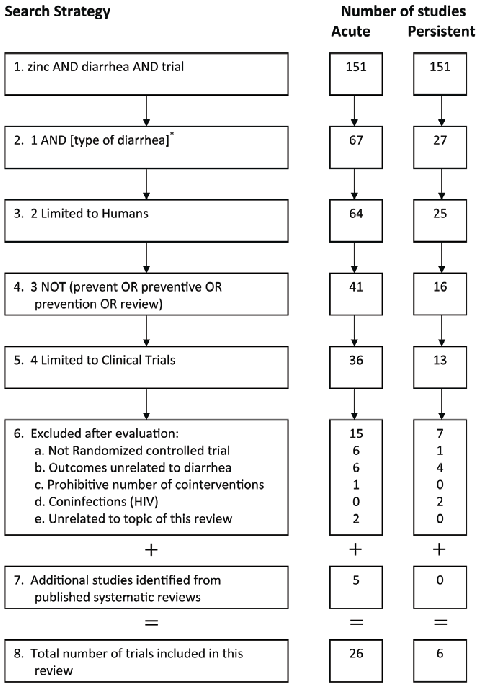
Figure 1
A PRISMA-style flowchart details the study selection protocol for this systematic review of zinc supplementation in diarrhea, showing the screening and inclusion criteria applied to identify eligible trials.
flowchart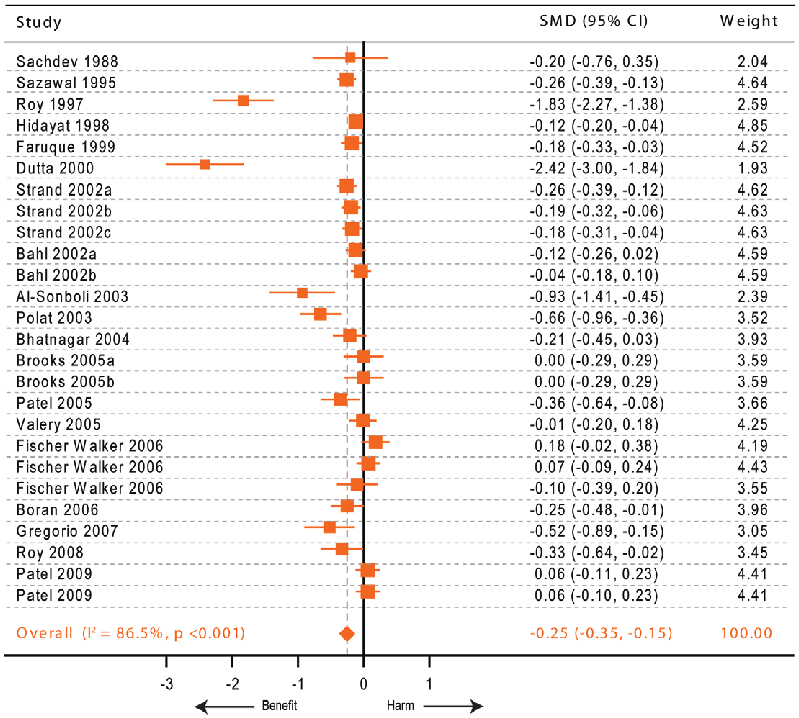
Figure 2
Subgroup comparisons of zinc dosage and formulation effects on diarrhea outcomes are depicted, highlighting dose-response relationships observed across studies.
chart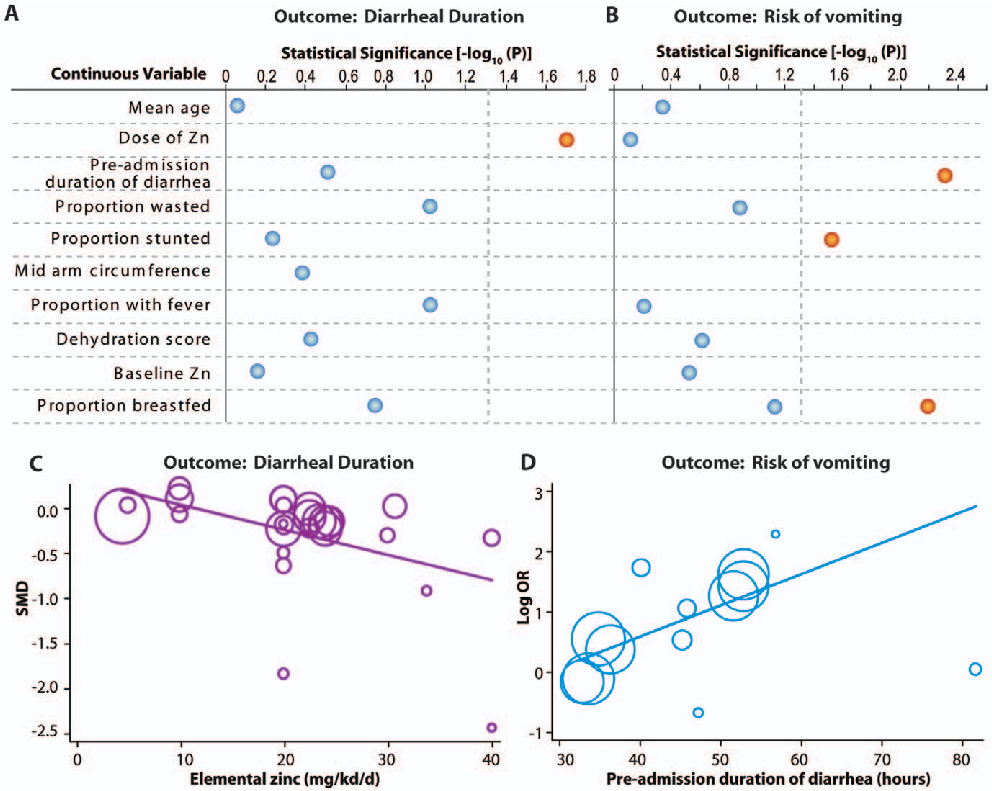
Figure 3
Pooled results from clinical trials assessing zinc's therapeutic value in reducing diarrhea duration and severity are presented, with subgroup analyses by diarrhea type.
chart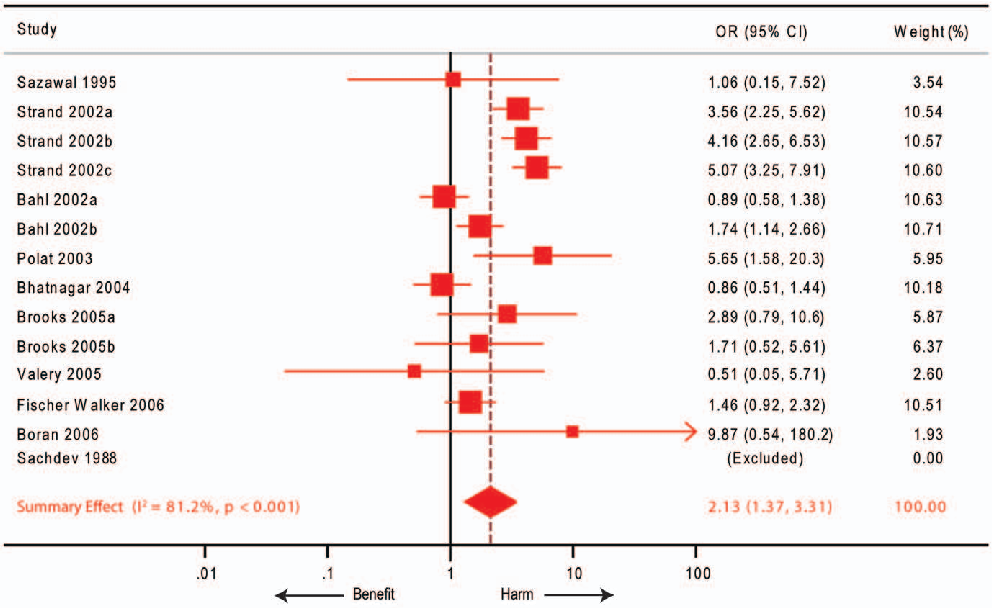
Figure 4
Effect size estimates for zinc supplementation across different age groups and diarrhea classifications are compared, indicating varying degrees of clinical benefit.
chartUsed In Evidence Reviews
Similar Papers
Advances in nutrition (Bethesda, Md.) · 2013
Discovery of human zinc deficiency: its impact on human health and disease.
The American journal of clinical nutrition · 2000
Therapeutic effects of oral zinc in acute and persistent diarrhea in children in developing countries: pooled analysis of randomized controlled trials.
The Journal of nutrition · 2003
Zinc deficiency, infectious disease and mortality in the developing world.
Food and nutrition bulletin · 2009
Preventive zinc supplementation among infants, preschoolers, and older prepubertal children.
The American journal of clinical nutrition · 1998
Therapeutic and preventive effects of zinc on serious childhood infectious diseases in developing countries.
Pediatrics · 2008