The Efficacy and Safety of Single-Strain Probiotic Formulations Containing Bifidobacterium lactis or Bacillus coagulans in Adult Patients with Irritable Bowel Syndrome-A Randomized Double-Blind Placebo-Controlled Three-Arm Interventional Trial.
Study Design
- Study Type
- Randomized Controlled Trial
- Population
- Adults with IBS
- Duration
- 12 weeks
- Intervention
- The Efficacy and Safety of Single-Strain Probiotic Formulations Containing Bifidobacterium lactis or Bacillus coagulans in Adult Patients with Irritable Bowel Syndrome-A Randomized Double-Blind Placeb 20.5%
- Comparator
- placebo
- Primary Outcome
- IBS symptom improvement
- Effect Direction
- Positive
- Risk of Bias
- Moderate
Abstract
Probiotics offer a potential new therapeutic approach for irritable bowel syndrome (IBS), but current results are still controversial. The aim of this study was to assess the efficacy and safety of single-strain probiotic formulations in adult IBS patients and to compare the effects of Bifidobacterium lactis NORDBIOTIC™ BI040 (DSM 33812/34614) and Bacillus coagulans NORDBIOTIC™ BC300 (DSM 33836) in a prospective three-arm interventional randomized double-blind placebo-controlled clinical trial. The study included 123 IBS subjects diagnosed according to the Rome IV criteria. The primary outcomes were changes in symptom severity and symptom improvement as assessed using the IBS Severity Scoring System (IBS-SSS) after 4, 8, and 12 weeks of intervention and after 4 weeks of follow-up. Secondary outcomes included the assessment of individual IBS symptoms and the occurrence of adverse events. During the 12-week intervention, IBS-SSS scores significantly decreased (p-values < 0.001) in the study groups but differences between the interventional and placebo groups did not reach statistical significance. However, at the 16th week of follow-up, a significant improvement in the total IBS-SSS score in comparison to the placebo group (20.5%) was found in 43.8% and 52.9% of the Bifidobacterium lactis (p = 0.038, OR 3.0, [95% CI 1.1-8.6]) and the Bacillus coagulans (p = 0.005, OR 4.6 [95% CI 1.5-12.2]) groups, respectively. Bifidobacterium lactis had a beneficial effect on the intensity and frequency of pain, whereas Bacillus coagulans decreased the bowel dissatisfaction. Both strains increased the percentage of patients with normal stool consistency, but only Bifidobacterium lactis induced a decrease in the number of patients with constipation after 6 weeks of supplementation. Both probiotic strains were well tolerated, without differences in the occurrence of adverse events between groups. In conclusion, single-strain supplementation was safe and efficient in IBS patients but showed a different range of effects. Bifidobacterium lactis BI040 primarily reduced the frequency and intensity of pain, while Bacillus coagulans BC300 increased bowel satisfaction [ClinicalTrials.gov NCT05064930].
TL;DR
In conclusion, single-strain supplementation was safe and efficient in IBS patients but showed a different range of effects, and both probiotic strains were well tolerated, without differences in the occurrence of adverse events between groups.
Full Text
Clinical Medicine
Article
The Efficacy and Safety of Single-Strain Probiotic Formulations Containing Bifidobacterium lactis or Bacillus coagulans in Adult Patients with Irritable Bowel Syndrome—A Randomized Double-Blind Placebo-Controlled Three-Arm Interventional Trial
Barbara Skrzydło-Radoman´ska 1, Beata Prozorow-Król 1, Anetta Kurzeja-Mirosław 1, Halina Cichoz-Lach˙ 1 , Katarzyna Laskowska 1, Emilia Majsiak 2 , Joanna B. Bierła 3 , Sowin´ska Agnieszka 3 and Bozena Cukrowska˙ 3,*
Citation: Skrzydło-Radoman´ska, B.; Prozorow-Król, B.; Kurzeja-Mirosław, A.; Cichoz-Lach, H.; Laskowska, K.;˙ Majsiak, E.; Bierła, J.B.; Agnieszka, S.; Cukrowska, B. The Efficacy and Safety of Single-Strain Probiotic Formulations Containing Bifidobacterium lactis or Bacillus coagulans in Adult Patients with Irritable Bowel Syndrome—A Randomized Double-Blind Placebo-Controlled Three-Arm Interventional Trial. J. Clin. Med. 2023, 12, 4838. https://doi.org/ 10.3390/jcm12144838
Academic Editors: Faming Zhang and Gianluca Ianiro
Copyright: © 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/).
- 1 Department of Gastroenterology, Medical University of Lublin, Jaczewskiego 8, 20-950 Lublin, Poland; [email protected] (B.S.-R.); [email protected] (B.P.-K.); [email protected] (A.K.-M.); [email protected] (H.C.-L.); [email protected] (K.L.)
- 2 Department of Health Promotion, Faculty Health of Sciences, Medical University of Lublin, Staszica 4/6, 20-081 Lublin, Poland; [email protected]
- 3 Department of Pathomorphology, The Children’s Memorial Health Institute, Aleja Dzieci Polskich 20, 04-730 Warsaw, Poland; [email protected] (J.B.B.); [email protected] (S.A.)
- 4 weeks of follow-up. Secondary outcomes included the assessment of individual IBS symptoms and the occurrence of adverse events. During the 12-week intervention, IBS-SSS scores significantly decreased (p-values < 0.001) in the study groups but differences between the interventional and placebo groups did not reach statistical significance. However, at the 16th week of follow-up, a significant improvement in the total IBS-SSS score in comparison to the placebo group (20.5%) was found in 43.8% and 52.9% of the Bifidobacterium lactis (p = 0.038, OR 3.0, [95% CI 1.1–8.6]) and the Bacillus coagulans (p = 0.005, OR 4.6 [95% CI 1.5–12.2]) groups, respectively. Bifidobacterium lactis had a beneficial effect on the intensity and frequency of pain, whereas Bacillus coagulans decreased the bowel dissatisfaction. Both strains increased the percentage of patients with normal stool consistency, but only Bifidobacterium lactis induced a decrease in the number of patients with constipation after 6 weeks of supplementation. Both probiotic strains were well tolerated, without differences in the occurrence of adverse events between groups. In conclusion, single-strain supplementation was safe and efficient in IBS patients but showed a different range of effects. Bifidobacterium lactis BI040 primarily reduced the frequency and intensity of pain, while Bacillus coagulans BC300 increased bowel satisfaction [ClinicalTrials.gov NCT05064930].
Keywords: irritable bowel syndrome; probiotics; Bifidobacterium lactis; Bacillus coagulans; IBS-SSS
1. Introduction
Irritable bowel syndrome (IBS) is one of the most commonly diagnosed functional gastrointestinal disorders and is characterized by recurrent abdominal pain and discomfort
J. Clin. Med. 2023, 12, 4838. https://doi.org/10.3390/jcm12144838 https://www.mdpi.com/journal/jcm
associated with changes in bowel frequency and/or stool consistency in the absence of an organic disease [1]. The global prevalence of IBS ranges from <5% up to 20%, depending on the country or region and the criteria used [2,3]. IBS is classified on the basis of the stool pattern as diarrhea-predominant (IBS-D), constipation-predominant (IBS-C), mixed bowel habits (IBS-M), and un-classified (IBS-U). IBS mostly starts in early adulthood and is more common among women than men [1].
IBS pathogenesis is multifactorial with a spectrum of abnormalities, including mucosal inflammation, increased intestinal permeability, altered gut motility, visceral hypersensitivity, small-bowel bacterial overgrowth (SIBO), compromised gut microbiome compromised gut microbiome, and impaired neuroendocrinal communications [4–8]. It is currently supposed that gut microbiota dysbiosis may be a potential trigger for IBS, inducing most of the pathological conditions [7,8]. Indeed, analyses of stool samples of IBS patients in comparison with healthy controls showed decreased proportions of the genera Bifidobacterium and Lactobacillus and increased ratios of the phylum Firmicutes: Bacteroidetes in most studies [9–11]. Thus, the modulation of dysbiotic intestinal microbiota by biologically active biotics including probiotics, prebiotics, and, when combined, as synbiotics, is a promising treatment approach in IBS. Probiotics are defined as live microorganisms that, when administrated at the proper dose, have beneficial effects on host health [12]. Prebiotics (most often oligosaccharides such as fructo-oligosaccharides (FOS) or galacto-oligosaccharides) are substrates that are selectively utilized by host microorganisms and probiotic strains conferring a health benefit [13]. Clinical trials indicate that probiotic or synbiotic administration is beneficial for IBS patients, but the efficacy of such therapies depends on probiotic strain selection [14–16]. Our research team evaluated a multi-strain probiotic formulation and a multi-strain synbiotic (a combination of probiotic strains with short-chain prebiotic FOS) formulation in two randomized double-blind placebo-controlled (RDBPC) clinical trials in patients with IBS-D [17,18]. The results indicated a beneficial effect of both formulations on the clinical course of IBS, assessed using the international IBS symptom severity scale (IBS-SSS), but with each of the study formulations exhibiting effectiveness in different fields. The formulation composed of a mixture of Bifidobacterium, Lactobacillus, and Streptococcus thermophilus strains significantly reduced pain severity and improved the quality of patients’ life [17], whereas the synbiotic formulation effectively improved bloating and had a beneficial effect on the general condition of the intestines [18]. A systematic review and meta-analysis published in 2020 showed that single-strain formulations, particularly those containing Bifidobacterium or Lactobacillus strains, may be more effective in IBS patients [14]. Other reports demonstrated high efficacy of a new-generation probiotic—the lactic acidproducing Bacillus coagulans [19]. Therefore, the main objective of the current study is to assess the efficacy and safety of the single-strain probiotic formulation in patients with IBS. We would like to compare the effects of two different probiotic strains, i.e., Bifidobacterium lactis NORDBIOTIC™ BI040 and Bacillus coagulans NORDBIOTIC™ BC300 in a prospective three-arm interventional RDBPC clinical trial.
2. Materials and Methods 2.1. Study Design
This was a prospective interventional RDBPC trial. The participants consisted of patients attending gastroenterology outpatient clinics between September 2021 and July 2022. The study was conducted in accordance with the ethical principles set out in the Declaration of Helsinki Guideline on Good Clinical Practice. The trial was approved by the Bioethics Committee at the Regional Medical Chamber in Lublin and was given decision number 173/202l/KB/VIII. The participants were informed of the purposes and conditions of the study and signed the relevant informed consent form. The patients were also informed of the option to refuse and withdraw their consent at any time, without stating the reason or suffering any consequences, and without losing the right to receive further care at the outpatient clinics or at the Department of Gastroenterology, Medical
conditions of the study and signed the relevant informed consent form. The patients were also informed of the option to refuse and withdraw their consent at any time, without
J. Clin. Med. 2023, 12, 4838 3 of 19
University of Lublin. The study was registered at ClinicalTrials.gov and received the trial number NCT05064930.
University of Lublin. The study was registered at ClinicalTrials.gov and received the trial number NCT05064930.
The study schedule included six visits: the screening visit, whose purpose was to qualify patients to be enrolled in the study; the baseline visit after up to 14 days following the screening visit, at which participants were randomized to the intervention groups; three follow-up visits after a 1-week run-in observation, held at weeks 4, 8, and 12 ± 3 days after starting the intervention; and the final follow-up visit after finishing the intervention at week 16. The last follow-up visit was a phone visit by the researchers; the other visits were at the clinics. The scheme of the study protocol is presented in Figure 1. After enrollment into the study, participants received a diary to fill out on a daily basis. Participants were also monitored weekly by interviewers by phone throughout the study.
The study schedule included six visits: the screening visit, whose purpose was to qualify patients to be enrolled in the study; the baseline visit after up to 14 days following the screening visit, at which participants were randomized to the intervention groups; three follow-up visits after a 1-week run-in observation, held at weeks 4, 8, and 12 ± 3 days after starting the intervention; and the final follow-up visit after finishing the intervention at week 16. The last follow-up visit was a phone visit by the researchers; the other visits were at the clinics. The scheme of the study protocol is presented in Figure 1. After enrollment into the study, participants received a diary to fill out on a daily basis. Participants were also monitored weekly by interviewers by phone throughout the study.
Figure 1. The flowchart of study protocol.
- 2.1.1. Patient Inclusion and Exclusion Criteria
- 2.1.1. Patient Inclusion and Exclusion Criteria
The study included female and male patients aged 18–70 years who were diagnosed with IBS according to the Rome IV criteria, i.e., patients with recurrent abdominal pain on average at least one day a week in the last three months, associated with two or more of the following: (1) related to defecation (either increasing or improving pain), (2) associated with a change in stool frequency, (3) associated with a change in stool form (appearance) [20]. Stool consistency was assessed with the Bristol Stool Form (BSF) scale [21]. Patients with the following IBS types were included: IBS-D (more than 25% of BSF type 6 and 7 stools and less than 25% of type 1 and 2 stools); IBS-C (more than 25% of BSF type 1 and 2 stools, with less than 25% of type 6 and 7 stools); IBS-M (more than 25% of BSF type 6 and 7 stools and also more than 25% of type 1 and 2 stools). IBS severity was assessed by the use of the IBS-SSS score [22]. Patients with at least a moderate type of IBS (IBS-SSS score > 175 points) were enrolled into the study.
The study included female and male patients aged 18–70 years who were diagnosed with IBS according to the Rome IV criteria, i.e., patients with recurrent abdominal pain on average at least one day a week in the last three months, associated with two or more of the following: (1) related to defecation (either increasing or improving pain), (2) associated with a change in stool frequency, (3) associated with a change in stool form (appearance) [20]. Stool consistency was assessed with the Bristol Stool Form (BSF) scale [21]. Patients with the following IBS types were included: IBS-D (more than 25% of BSF type 6 and 7 stools and less than 25% of type 1 and 2 stools); IBS-C (more than 25% of BSF type 1 and 2 stools, with less than 25% of type 6 and 7 stools); IBS-M (more than 25% of BSF type 6 and 7 stools and also more than 25% of type 1 and 2 stools). IBS severity was assessed by the use of the IBS-SSS score [22]. Patients with at least a moderate type of IBS (IBS-SSS score > 175 points) were enrolled into the study.
The exclusion criteria were subjects aged <18 and >70 years; unclassified IBS; gastrointestinal conditions other than IBS, such as inflammatory bowel diseases, celiac disease, gastroenteritis, gastric and duodenal ulcers; constipation; parasitic or bacterial intestinal infestation/infections; diagnosed lactose intolerance; hypersensitivity to food allergens; coexisting severe diseases such as malignancies, uncontrolled hypertension (blood pressure > 170/100 mmHg), uncontrolled diabetes mellitus (fasting blood glucose > 11 mmol/L), serious neurological disorders, psychosis, respiratory disorders (asthma, chronic obstructive
The exclusion criteria were subjects aged <18 and >70 years; unclassified IBS; gastrointestinal conditions other than IBS, such as inflammatory bowel diseases, celiac disease,
pulmonary disease), hyper- or hypothyroidism, and hepatic, renal or cardiac dysfunctions; pregnancy or breastfeeding; being on gluten-free and low FODMAP (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols) diets; antibiotic therapy during the 1 month preceding the study; the current use of dietary supplements or drugs targeting the gut microbiota, such as probiotics, prebiotics, synbiotics, and short chain fatty acids, and refusal to undergo a 1-month washout period. Other exclusion criteria included the use of motility medications or dietary fiber supplements within 2 weeks before the study start, taking anti-coagulant drugs, plans to have surgery during the time of the study, a history of alcohol or drug abuse, and participation in another clinical trial during the 3 months prior the study entry. Patients who were treated with antibiotics during the study were also excluded. Patients were allowed to take spasmolytic drugs on an ad hoc basis and/or the low-dose antidepressants amitriptyline, nortriptyline or selective serotonin inhibitor at up to 25 mg per day.
Withdrawal criteria after enrollment into the study included compliance with probiotic or placebo supplementation of below 80%, non-attendance at the study visits, non-contact with the telephone interviewer, exclusion criteria found after enrollment, and any serious adverse event during the intervention period.
- 2.1.2. Intervention
- 2.1.3. The Study Protocol
During screening visits, the patients underwent physical examination to establish the presence of clinical inclusion criteria. Out of 223 patients with IBS, 196 met the inclusion criteria for age and IBS severity (IBS-SSS score > 175), with 45 of them not meeting some of the other inclusion criteria and a further 31 not agreeing to participate in the study (Figure 1). Finally, 120 patients meeting all inclusion criteria signed the informed consent form and were enrolled into the trial. All participants were instructed on how to assess the symptoms about which they would be asked by telephone interviewers and were trained not to consume foods and dietary supplements containing probiotics/synbiotics or other active agents influencing the gut microbiota according to the exclusion criteria. During the first baseline visit, patients were allocated to groups A, B, or C according to a computergenerated randomization list with the use of the web page https://www.random.org/lists “URL (accessed on 20 August 2021)”. The randomization was blinded to both patients and researchers. At the baseline visit, the researchers informed participants not to take the product for the first week (7 days run-in observation) and to complete a diary daily (containing information about the number and type of stool and the severity of specific IBS symptoms); on the 7th day, a telephone interviewer informed the participant to start taking the product from the next day onwards. Patients were asked to take orally one capsule a day over a 12-week period. Patients reported to a researcher every 4 weeks in order to receive the probiotic preparation or placebo for the next 4 weeks and to be clinically
assessed. The telephone interviewers called patients once a week and reminded patients to fill out diaries daily, and they also collected information on the IBS symptoms, drugs taken, and the occurrence of any adverse events. The telephone interviewers were recruited from among the research staff of the Department of Pathomorphology, the Children’s Memorial Health Institute in Warsaw.
- 2.1.4. Outcome Definitions
The primary outcomes included an assessment of IBS severity with the use of the IBSSSS score and any improvement of clinical symptoms. IBS-SSS is a 5-question survey about the severity of abdominal pain (IBS-SSS1), the number of days with abdominal pain over the last 10 days (IBS-SSS2), the severity of abdominal distension (IBS-SSS3), dissatisfaction with bowel habit (IBS-SSS4), and interference with the quality of life over the past 10 days (IBS-SSS5) [22]. The number of days with pain was multiplied by 10. Each of the five questions generate a maximum score of 100 points, and total scores ranged from 0–500, with higher scores indicating severe symptoms. A drop of at least 2 scoring categories (at least 50%) compared with the baseline was assumed to be associated with a clinically meaningful improvement. In the case of the number of days with pain, a decrease below at least 2 standard deviations was considered an improvement.
Secondary outcomes included changes in stool consistency evaluated using the BSF scale, the number of bowel movements per day, the severity of pain and flatulence, fecal urgency, the feeling of incomplete stool evacuation, and the effect of intervention on the occurrence of adverse events. The data were collected from patients’ diaries and telephone interviewers. IBS symptoms, except for the sensation of incomplete bowel movements, were assessed using a patient-defined 5-point Likert’s scale as was described in our previous paper [18]. Briefly, a score of 0 indicated no symptoms, and scores of 1–4 were based on the severity of symptoms; the higher the score, the more severe the symptoms. A feeling of incomplete bowel movement was assessed using a 2-point scale: 0 = no such feeling and 1 = there is an incomplete bowel movement. Adverse events and the taking of drugs were evaluated as either 0 = no or 1 = yes.
- 2.2. Statistics
The Stata Program version 16.0 was used for statistical analysis. Differences between the groups in nominal variables (e.g., sex, the number of patients with an improvement, adverse events, the absence or presence of specific symptoms) were evaluated with the use of Fisher’s exact test. In the case of continuous variables (e.g., age, physical development parameters, IBS-SSS scores, the duration of adverse events), ANOVA and Repeated Measures ANOVA (RM-ANOVA) were used if the normality of residuals assumption held. The normality of distribution of residuals was analyzed by the Shapiro–Wilk test. When the assumption of the normal distribution of residuals did not hold, the Kruskal–Wallis multiple comparison test and the Scheirer–Ray–Hare test were used. In the follow-up analysis of the pairwise comparisons, the Wilcoxon rank-sum test was applied. The threshold of significance for all analyses was set to α = 0.05. In the follow-up analysis of the pairwise comparisons, the p-values were adjusted with the use of the Bonferroni or Benjamini– Hochberg methods.
To reduce the dimension of the dataset from the patients’ diary (day) level, the data were transformed to weekly level observations. For all variables, except for a feeling of incomplete bowel movement and adverse events, the mean (average) value for each week was calculated. For a feeling of incomplete bowel movement, coded as a dummy variable taking values 0 or 1, the most common value was calculated for each week (mode). For side effects, two measures were calculated: (1) a variable for the presence of the adverse events at a week level (no matter how many days), and (2) the duration of side effects expressed as the number of days the side effect was observed during each week. In the second step, the scales used in diaries were transformed as follows: type of stools
(1 = normal, 0 = constipation, or 2 = diarrhea), intensity of pain, flatulence, or fecal urgency (0 = no symptoms, 1 = moderate, or 2 = severe).
- 3. Results 3.1. Patients
A total of 123 patients were randomized to receive the probiotic preparation or the placebo (Figure 1). After the 12-week intervention period, 7 patients from the Bifidobacterium lactis-supplemented group dropped out of the study due to antibiotics use (n = 2), hospital stay (n = 1), COVID-19 infection (n = 1), lack of contact with the interviewer (n = 1), and resignation due to no improvement (n = 2), while 6 patients dropped out of the Bacillus coagulans-supplemented group due to antibiotics use (n = 3), lack of contact with the interviewer (n = 2), and resignation due to no improvement (n = 1). Four patients from the placebo group dropped out due to antibiotics use (n = 2) and resignation due to no improvement (n = 2).
A final total of 106 patients (86.7% of enrolled patients) finished the study. Characteristics of the patients are shown in Table 1. Females were predominant in all groups. The mean age of the patients ranged from 39.5 ± 13.8 years in the placebo group to 40.8 ± 13.2 in the Bifidobacterium lactis group and 39.0 ± 17.0 years in the Bacillus coagulans group. Most often, patients were diagnosed with IBS-M and IBS-D. The IBS-D type was most commonly observed in the Bacillus coagulans group (50.0%), while the IBS-M type was most common in the Bifidobacterium lactis and placebo groups, comprising 42.4% and 58.9% of the patients, respectively. Patients with severe IBS (with IBS-SSS score > 300 points) predominated in all groups, accounting for 76.9% in the placebo group, 69.7% in the Bifidobacterium lactis group, and 76.5% in the Bacillus coagulans group. Statistical analysis showed no statistically significant differences between the study groups in terms of patient sex, age, physical development, type of IBS, or IBS severity.
Table 1. Patients’ characteristics.
Bifidobacterium lactis NORDBIOTIC™ BI040 Group (n = 33) n (%) or Mean ± SD
Bacillus coagulans NORDBIOTIC™ BC300 Group (n = 34) n (%) or Mean ± SD
Control Group (n = 39) N (%) or Mean ± SD
Gender Female 33 (84.6%) 21 (63.6%) 23 (67.4%)
Male 6 (15.4%) 11 (33.3%) 11 (32.6%)
Age in years 39.5 ± 13.8 40.8 ± 13.2 39.0 ± 17.0 Height (m) 1.68 ± 0.08 1.70 ± 0.13 1.69 ± 0.1
Body weight (kg) 67.0 ± 15.6 74.0 ± 16.9 70.8 ± 13.9 BMI 23.5 ± 4.2 25.7 ± 5.5 24.6 ± 4.5
IBS type IBS-D 12 (30.8%) 12 (36.4%) 17 (50.0%) IBS-C 4 (10.3%) 7 (21.2%) 4 (11.7%) IBS-M 23 (58.9%) 14 (42.4%) 12 (35.3%)
IBS severity * Moderate 9 (23.1%) 10 (30.3%) 8 (23.5%) Severe 30 (76.9%) 23 (69.7%) 26 (76.5%)
Total IBS-SSS score 349.7 ± 58.0 344.4 ± 63.9 335.8 ± 65.1
* IBS severity was assessed based on the IBS-SSS scale. There were no significant statistical differences between patients receiving probiotic preparations and the placebo control group. BMI = Body Mass Index. Severe IBS is when the IBS-SSS score is >300, moderate IBS is when IBS-SSS score is >175 and ≤300. SD = standard deviation.
3.2. The Effect of Probiotic Supplementation on the IBS-SSS Score
The primary outcomes included changes in IBS symptom severity as evaluated with the use of the IBS-SSS score. The mean values of the total IBS-SSS score before the in-
tervention were similar in all the study groups, being 349.7 ± 58.0, 344.4 ± 63.9 and 335.8 ± 65.1 in the placebo, Bifidobacterium lactis and Bacillus coagulans groups, respectively (Table 2). During the 12-week intervention, IBS-SSS scores steadily and significantly decreased (p-values < 0.001) in both the probiotic-supplemented groups (to 167.8 ± 85.8 and 184.2 ± 97.4 in the Bifidobacterium lactis and the Bacillus coagulans groups, respectively) and in the placebo group (180.5 ± 81.9). The observed strong placebo effect resulted in no statistically significant differences between the groups with the probiotic intervention and the control group, except for a statistically significant reduction in pain frequency after 4 weeks of intervention in the Bifidobacterium lactis group compared with the placebo group (p-value = 0.013). The average number of days with pain during last 10 days in the Bifidobacterium lactis-supplemented group decreased from 6.8 before the intervention to 3.7, while in the placebo group, it was 7.0 and 5.5, respectively. This decrease was maintained throughout the intervention period (12 weeks) and after its completion. At week 16 (4 weeks after the end of the intervention), the Bifidobacterium lactis group had a mean number of pain days of 2.6, which was significantly (p-value = 0.008) lower compared with the placebo group, where pain was reported for an average of 4.6 days. Interestingly, the number of days with pain in the Bifidobacterium lactis group at the 16-week follow-up observation was statistically significantly fewer even compared with the group supplemented with the Bacillus coagulans strain, in which the average number of pain-free days was 3.9 (p-value = 0.042). Bifidobacterium lactis BI040 supplementation also had a significant effect on pain intensity. In the 16th week of follow-up observation, the IBS-SSS2 pain intensity score was significantly lower in the Bifidobacterium lactis group compared with the placebo group (p-value = 0.026) and amounted to 25.0 ± 19.4 and 37.8 ± 19.8 points, respectively.
In the 16th week of the trial, i.e., 4 weeks after the end of the intervention, a decrease in the IBS-SSS scores compared with the baseline was observed in all study groups, but at the same time, an increase in the scoring, indicating a worsening of the clinical condition compared with week 12, i.e., the end of the intervention, was found. However, this increase in scores was primarily seen in the placebo group. Compared with the end of the intervention, the average total IBS-SSS score in the follow-up observation increased by 55.8 points in the placebo group, while it increased by 28.6 points in the Bifidobacterium lactis group and only by 8.6 points in the Bacillus coagulans group. The beneficial effect of probiotic supplementation after the end of intervention during the follow-up period was observed mainly in terms of the intensity and frequency of pain in the Bifidobacterium lactis group described above, and of the dissatisfaction with the bowel habit in the Bacillus coagulans group. Four weeks after the end of the intervention, bowel dissatisfaction was rated at an average of 47.0 points in the Bacillus coagulans-supplemented group, while in the placebo group, it was as high as 59.4 points (p-value = 0.044).
Table 2. The effect of probiotic intervention on the severity of IBS symptoms assessed with the use of IBS-SSS scores.
Follow-up after the End of Intervention (16 Weeks)
Baseline 4 Weeks of Intervention 8 Weeks of Intervention 12 Weeks of Intervention
Groups
p-Value between Groups
p Value between Groups
p-Value between Groups
p-Value between Groups IBS-SSS total score
Mean ± SD Mean ± SD
Mean ± SD
Mean ± SD
Mean ± SD
Placebo (P) 349.7 ± 58.0 277.6 ± 72.2 Bl vs. P: NS 224.7 ± 77.7 BI vs. P: NS 180.5 ± 81.9 BI vs. P: NS 236.3 ± 97.4 BI vs. P: NS Bifidobacterium lactis BI040 (BI)
344.4 ± 63.9 241.1 ± 69.2 BC vs. P: NS 214.5 ± 80.2 BC vs. P: NS 167.8 ± 85.8 BC vs. P: NS 196.4 ± 89.6 BC vs. P: NS Bacillus coagulans BC300 (BC)
335.8 ± 65.1 248.1 ± 89.8 Bl vs. BC: NS 212.7 ± 90.2 BI vs. BC: NS 184.2 ± 97.4 BI vs. BC: NS 192.8 ± 88.1 BI vs. BC: NS
IBS-SSS1 score (the intensity of pain)
Placebo (P) 55.1 ± 19.2 39.1 ± 18.0 BI vs. P: NS 31.4 ± 17.9 BI vs. P: NS 24.4 ± 16.7 BI vs. P: NS 37.8 ± 19.8 * BI vs. P: 0.026 Bifidobacterium lactis BI040 (BI)
47.7 ± 17.0 29.6 13.2 BC vs. P: NS 26.5 ± 14.0 BC vs. P: NS 22.7 17.0 BC vs. P: NS 25.0 ± 19.4 BC vs. P: NS Bacillus coagulans BC300 (BC)
49.3 ± 22.6 35.3 ± 21.4 BI vs. BC: NS 32.4 ± 20.0 BI vs. BC: NS 25.7 ± 19.9 BI vs. BC: NS 29.6 ± 22.9 BI vs. BC: NS
IBS-SSS2 score (the frequency of pain)
Placebo (P) 70.0 ± 25.1 55.4 ± 24.9 * BI vs. P: 0.013 44.1 ± 32.3 BI vs. P: NS 33.3 ± 28.9 BI vs. P: NS 46.1 ± 30.1 * BI vs. P: 0.008 Bifidobacterium lactis BI040 (BI)
68.5 ± 27.3 37.6 ± 27.9 BC vs. P: NS 33.9 ± 26.0 BC vs. P: NS 23.9 ± 24.6 BC vs. P: NS 26.1 ± 18.9 BC vs. P: NS Bacillus coagulans BC300 (BC)
66.8 ± 26.7 49.1 ± 29.7 BI vs. BC: NS 42.1 ± 26.7 BI vs. BC: NS 33.5 ± 26.8 BI vs. BC: NS 39.1 ± 24.3 * BI vs. BC: 0.042
IBS-SSS3 score (the severity of flatulance)
Placebo 69.9 ± 28.2 50.0 ± 27.5 BI vs. P: NS 41.7 ± 19.3 BI vs. P: NS 31.4 ± 19.6 BI vs. P: NS 37.8 ± 22.8 BI vs. P: NS Bifidobacterium lactis BI040 (BI)
70.4 ± 26.1 47.7 ± 24.5 BC vs. P: NS 43.9 ± 25.0 BC vs. P: NS 31.1 ± 17.7 BC vs. P: NS 38.7 ± 24.0 BC vs. P: NS Bacillus coagulans BC300 (BC)
67.6 ± 22.6 47.1 ± 26.7 BI vs. BC: NS 35.3 ± 23.1 BI vs. BC: NS 31.6 ± 24.8 BI vs. BC: NS 31.1 ± 17.7 BI vs. BC: NS
IBS-SSS4 score (dissatisfaction with bowel habit)
Placebo (P) 79.9 ± 16.9 68.7 ± 19.5 BI vs. P: NS 52.5 ± 18.2 BI vs. P: NS 46.6 ± 22.4 BI vs. P: NS 59.4 ± 24.4 BI vs. P: NS
Table 2. Cont.
Follow-up after the End of Intervention (16 Weeks)
Baseline 4 Weeks of Intervention 8 Weeks of Intervention 12 Weeks of Intervention
Groups
p-Value between Groups
p-Value between Groups
p Value between Groups
p-Value between Groups Bifidobacterium lactis BI040 (BI)
Mean ± SD Mean ± SD
Mean ± SD
Mean ± SD
Mean ± SD
81.4 ± 17.2 62.1 ± 18.2 BC vs. P: NS 56.1 ± 19.5 BC vs. P: NS 46.0 ± 20.1 BC vs. P: NS 51.2 ± 26.8 * BC vs. P: 0.044 Bacillus coagulans BC300 (BC)
80.0 ± 18.9 60.3 ± 20.9 BI vs. BC: NS 54.4 ± 23.0 BI vs. BC: NS 47.6 ± 26.1 BI vs. BC: NS 47.0 ± 18.5 BI vs. P: NS
IBS-SSS5 score (quality of life)
Placebo (P) 74.7 ± 15.0 64.4 ± 15.2 BI vs. P: NS 55.0 ± 20.6 BI vs. P: NS 44.9 ± 24.6 BI vs. P: NS 55.1 ± 26.8 BI vs. P: NS Bifidobacterium lactis BI040 (BI)
76.3 ± 17.9 64.1 ± 18.6 BC vs. P: NS 54.1 ± 24.6 BC vs. P: NS 44.0 ± 27.0 BC vs. P: NS 55.4 ± 19.9 BC vs. P: NS Bacillus coagulans BC300 (BC)
72.1 ± 17.6 56.4 ± 23.9 BI vs. BC: NS 48.6 ± 27.3 BI vs. BC: NS 45.7 ± 28.3 BI vs. BC: NS 46.1 ± 24.8 BI vs. BC: NS
IBS symptoms were evaluated with the use of the IBS-SSS scores at baseline, 4th, 8th, and 12th week of the intervention, and at 4 weeks after the end of the intervention (16th week of the study). The table shows mean values of the IBS-SSS scores ± standard deviations (SD). A score reduction corresponded to symptom amelioration. * Statistically significant p-values (p < 0.05). NS = not significant.
3.3. The Effect of Probiotic Intervention on Clinical Improvement
An improvement in clinical symptoms, defined as a drop in IBS-SSS scores by at least two scoring categories (at least by 50%) or a decrease the number of days without pain by 2 standard deviations compared with the baseline observation, was a primary endpoint of the current study. The effect of intervention on clinical improvement is presented in Figure 2, and detailed statistical analysis for significant results involving odds ratio (OR) and 95% confidence interval (CI) is shown in Table 3.
*
*
* *
#
*
The effect of probiotic intervention on clinical improvement assessed by IBS-SSS scores (a–f). * indicates a statistically significant improvement ( between both the groups given probiotic intervention and the placebo group in the total IBS-SSS score (a), and between the Bifidobacterium lactis
Table 3. The effect of probiotic intervention on the improvement of IBS symptoms assessed by the total IBS-SSS score and IBS-SSS2 score.
4 Weeks of Intervention 8 Weeks of Intervention 12 Weeks of Intervention Follow-Up (16 Weeks) p-Value OR (95% CI) p-Value OR (95% CI) p-Value OR (95% CI) p-Value OR (95% CI)
Groups
An improvement in clinical symptoms assessed by total IBS-SSS score
Bifidobacterium lactis BI040 vs. placebo
NS 2.4 (0.5–10.9) NS 1.1 (0.4–3.2) NS 1.2 (04–3.0) * 0.038 3.0 (1.1–8.6) Bacillus coagulans BC300 vs. placebo
NS 2.7 (0.6–12.1) NS 1.2 (0.4–3.4) NS 0.8 (0.3–2.1) * 0.005 4.6 (1.5–12.2)
An improvement in pain frequency assessed by IBS-SSS2 score
Bifidobacterium lactis BI040 vs. placebo
* 0.020 12.7 (1.5–107.7) NS 1.8 (0.6–5.5) * 0.038 3.0 (1.1–8.6) * 0.010 4.3 (1.4–13.0) Bacillus coagulans BC300 vs. placebo
NS 5.1 (05–47.7) NS 0.8 (0.2–2.7) NS 1.8 (0.6–5.3) 0.054 3.0 (0.98–9.2)
The table shows the exact statistical analysis including p-value, odds ratio (OR) and 95% confidence interval (CI) of the clinical improvement (a decrease in IBS-SSS scores by at least 50% compared with baseline) between the groups with probiotic intervention and the placebo group. Only the analysis of parameters that showed statistically significant differences, i.e., total IBS-SSS score and the IBS-SSS2 score evaluating the frequency of pain. Clinical assessment using the IBS-SSS1, IBS-SSS3, IBS-SSS4, and IBS-SSS5 scores did not show any statistical differences between the study groups. * Statistically significant p-values (p < 0.05). NS = not significant.
Statistically significant differences between study groups in an improvement was found for the total IBS-SSS score and the IBS-SSS2 score evaluating the frequency of pain (Table 3). A significant improvement in global clinical symptoms assessed with the total IBS-SSS score in comparison with the placebo group was observed in both probioticsupplemented groups after the end of the intervention at the 16th week of the trial. At this follow-up visit, 52.9% and 43.8% of the Bacillus coagulans-supplemented (p = 0.005, OR 4.6 [95% CI 1.5–12.2]) and Bifidobacterium lactis-supplemented (p = 0.038, OR 3.0 [95% CI 1.1–8.6]) groups, respectively, reported clinical improvement compared with 20.5% in the placebo group. A significant improvement in the number of days with pain was observed after 4 weeks (p = 0.02, OR 12.7 [95% CI 1.5–107.7]) and 12 weeks (p = 0.038, OR 3.0 [95% CI 1.1–8.6]) of intervention only in the Bifidobacterium lactis group compared with the placebo group. This positive effect was maintained for a further 4 weeks after the end of the intervention (p = 0.01, OR 4.3 [95% CI 1.4–13.0]). Patients from the Bacillus coagulans group also reported an improvement in the frequency of pain during the follow-up visit at the 16th week of the trial, reaching a p-value of 0.054 (OR 3.0 [95% CI 0.98–9.2]) compared with the placebo group.
3.4. The Effect of Intervention on Secondary Outcomes
Secondary outcomes included daily data reported by the patients in their diaries. Patients assessed the frequency and consistency of their stool, the severity of pain and flatulence, fecal urgency, and the feeling of incomplete evacuation of stool. In addition, telephone interviewers checked the completion of the diaries once a week. The percentage of returned diaries was as follows: in the placebo group, 84.6%; in the group supplemented with Bifidobacterium lactis, 69.7%; and in the group supplemented with Bacillus coagulans, 82.4%. The results confirmed the beneficial effect of Bifidobacterium lactis on the pain feeling (Figure 3 and Table 4). At the baseline week (week 0), all patients but one in the Bacillus coagulans group reported the presence of pain. During the intervention, only in the Bifidobacterium lactis group did the percentage of patients with no pain increase, reaching a statistically significant difference in comparison with the placebo group at week 9 (p = 0.047, OR 19.92 [95% CI 1.04–380.67]). At the 5th and 16th weeks of follow-up observation, the p-value between the groups was 0.07 (OR 15.46 [95% CI 0.79–302.78]) and 0.051 (OR 4.37 [95% CI 0.99–19.26]), respectively (Table 4). In contrast, such a beneficial effect on the pain feeling was not observed in the group supplemented with Bacillus coagulans. There were no significant differences in the intensity of pain (severe or moderate) between the study groups.
Figure 3. The effect of probiotic intervention on the intensity of pain, assessed using Likert’s scales (a–c), and the stool consistency, assessed with the Bristol Stool Formation scale (d–f). Data were reported daily in the patients’ diaries. * indicates statistically significant (p < 0.05) differences between the probiotic groups and the placebo group. # p-value < 0.08 and >0.05 between the probiotic groups and the placebo group. The black arrows show the duration of the intervention.
Figure 3. The effect of probiotic intervention on the intensity of pain, assessed using Likert’s scales (a–c), and the stool consistency, assessed with the Bristol Stool Formation scale (d–f). Data were reported daily in the patients’ diaries. * indicates statistically significant (p < 0.05) differences between the probiotic groups and the placebo group. # p-value < 0.08 and >0.05 between the probiotic groups and the placebo group. The black arrows show the duration of the intervention.
Table 4. The effect of probiotic intervention on secondary outcomes, presenting statistical differences in comparison with the placebo.
OR [95% CI] p-Value
Bacillus coagulans
Bifidobacterium lactis NORDBIOTIC™ BI040 Group (BI) n = 23
Placebo Group (P) n = 33
NORDBIOTIC™ BC300 Group (BC) n = 27
Symptoms
BI vs. P BC vs. P The pain intensity at 5th week of intervention
15.46 [0.79–302.78] p = 0.07
No pain 4 (17.4%) 2 (7.4%) 0
NS
Severe 0 5 (18.5%) 0 NS NS Moderate 19 (82.6%) 20 (74.1%) 33 (100%) NS NS
The pain intensity at 9th week of intervention
19.92 [1.04–380.67] p = 0.047
No pain 5 (21.7%) 3 (11.1%) 0
NS
Severe 1 (4.3%) 2 (7.4%) 2 (6.1%) NS NS Moderate 17 (74.0%) 22 (81.5%) 31 (93.9%) NS NS
The pain intensity at 16th week of the trial (4 weeks after the end of the intervention)
4.37 [0.99–19.26] p = 0.051
No pain 7 (30.4%) 2 (7.4%) 3 (9.1%)
NS
Severe 1 (4.3%) 5 (18.5%) 2 (6.1%) NS NS Moderate 15 (65.2%) 20 (74.1%) 28 (84.8%) NS NS
Type of stool at 6th week of intervention
7.91 [2.10–29.83] p = 0.002
4.98 [1.36–18.23] p = 0.015
Normal 12 (52.2%) 11 (40.7%) 4 (12.1%)
0.24 [0.08–0.73] p = 0.01
Constipation 7 (30.4%) 11 (40.7%) 20 (60.6%)
NS
Diarrhea 4 (17.4%) 5 (18.5%) 9 (27.3%) NS NS
The table shows the number and the percentage (in brackets) of patients reporting symptoms (the intensity of pain and the stool consistency) that showed statistical significant differences between groups supplemented with probiotics and the placebo group, the odds ratio (OR) and the 95% confidence interval [CI]. Data were reported daily in patients’ diaries. The intensity of pain was assessed using Likert’s scales and the stool consistency with the Bristol Stool Formation scale. Other symptoms assessed as secondary outcomes (the intensity of flatulence, fecal urgency, and the feeling of incomplete evacuation of stool) did not show statistical significantly differences between the study groups during the 16 weeks of observations and are not presented. NS = not significant.
Probiotic intervention resulted also in a significant improvement of stool consistency
- as assessed with the use of the BSF scale, which was observed at the 6th week of intervention (Figure 3, Table 4). The percentage of patients who reported normal stool consistency significantly increased in both supplemented groups compared with the placebo group
- at week 6 and was 52.2% in the Bifidobacterium lactis group (p = 0.002, OR 7.91 [95% CI
- 2.10–29.83]), 40.7% in the Bacillus coagulans group (p = 0.015, OR 4.98 [95% CI 1.36–18.23]), and only 12.1% in the placebo group. In addition, probiotic intervention with Bifidobacterium lactis significantly decreased the number of patients with constipation at the 6th week of intervention compared with the placebo (p = 0.01, OR 0.24 [95% CI 0.08–0.73]). Probiotic intervention did not affect the occurrence of diarrhea at that period of intervention. Other secondary outcomes (the number of stools per day, the intensity of flatulence,
Adverse events were reported in the patient’s diaries, and the data were collected by telephone interviewers. The data obtained from both sources were converged and
fecal urgency, and the feeling of incomplete evacuation of stool) were not affected by the probiotic interventions.
Bifidobacterium lactis BI040 and
- 3.5. Safety and Adverse Events
were safe and well tolerated. There were no statistically significant differences in the percentage of patients reporting adverse events between the study groups (Figure 4). Interestingly, patients supplemented with Bifidobacterium lactis reported a shorter duration of adverse events in comparison with the placebo group (p = 0.05) as well as with the Bacillus
Adverse events were reported in the patient’s diaries, and the data were collected by the telephone interviewers. The data obtained from both sources were converged and showed that both the Bifidobacterium lactis BI040 and Bacillus coagulans BC300 probiotics were safe and well tolerated. There were no statistically significant differences in the percentage of patients reporting adverse events between the study groups (Figure 4). Interestingly, patients supplemented with Bifidobacterium lactis reported a shorter duration of adverse events in comparison with the placebo group (p = 0.05) as well as with the Bacillus coagulans group (p = 0.042). The mean number of days with adverse events in the Bifidobacterium lactis group was 2.5 ± 1.9, whereas in the placebo group, it was 3.7 ± 2.0, and in the Bacillus coagulans group, it was 3.8 ± 2.4 (Figure 4).
0.042). The mean number of days with adverse events in the Bifidobacgroup was 2.5 ± 1.9, whereas in the placebo group, it was 3.7 ± 2.0, and in the
group, it was 3.8 ± 2.4 (Figure 4).
Figure 4. The percentage of patients reporting adverse events (a) and the mean number of days with adverse events (b) during an intervention period.
The percentage of patients reporting adverse events (a ) during an intervention period.
4. Discussion
Probiotics are potentially a promising approach in the treatment of functional bowel disorders, including IBS; however, discussions about their efficacy, dose, and composition are ongoing. The efficacy and safety of the use of probiotic products for IBS are supported by an increasing number of RDBPC studies. However, meta-analyses of these clinical trials do not give a clear answer as to which probiotics can be recommended in the treatment of IBS [14–16,19]. A meta-analysis of 37 RDBPC trials with 4403 patients published by Ford et al. in 2018 presented evidence for the use of combinations of probiotics as a group for improving global IBS symptoms and abdominal pain [15]. They also presented a trend toward a beneficial effect of Bifidobacterium strains. In terms of single-strain probiotics, Lactobacillus plantarum DSM 9843, Escherichia coli DSM1752, and Streptococcus faecium appeared to be beneficial, but the authors emphasized that the latter two were only used in one RDBPC trial. Xie et al. tried to evaluate the most effective combinations and components among different probiotics through a network meta-analysis of 65 clinical trials [23]. Standard network meta-analyses showed that Lactobacillus and Bifidobacterium strains were the most effective for the relief of global IBS symptoms and an improvement in abdominal pain. Component network meta-analyses showed that Bacillus and Lactobacillus were among the most effective components. A recently published network meta-analysis by Zhang et al. of 43 RDPC trials with 5531 IBS patients comparing different species showed that Bacillus coagulans exhibited the highest probability of being the optimal probiotic species
Probiotics are potentially a promising approach in the treatment of functional bowel disorders, including IBS; however, discussions about their efficacy, dose, and composition are ongoing. The efficacy and safety of the use of probiotic products for IBS are supported by an increasing number of RDBPC studies. However, meta-analyses of these clinical trials do not give a clear answer as to which probiotics can be recommended in the treatment of IBS [14–16,19]. A meta-analysis of 37 RDBPC trials with 4403 patients published by Ford et al. in 2018 presented evidence for the use of combinations of probiotics as a group for improving global IBS symptoms and abdominal pain [15]. They also presented a trend toward a beneficial effect of Bifidobacterium strains. In terms of single-strain probiotics, Lac-
DSM 9843, Escherichia coli DSM1752, and Streptococcus faecium appeared to be beneficial, but the authors emphasized that the latter two were only used in one RDBPC trial. Xie et al. tried to evaluate the most effective combinations and components among different probiotics through a network meta-analysis of 65 clinical trials [23].
for improving the IBS symptom relief rate as well as global symptoms, abdominal pain, bloating, and straining scores [19]. In addition, Bacillus coagulans had also significant efficacy compared with different types of probiotic combinations. Although different species and combinations of probiotics used in clinical trials were evaluated in the network meta-analyses, there are exceptions where studies compared the effectiveness of different species/strains during the one clinical trial [24]. That is why we decided to compare the effectiveness of two single-strain probiotic preparations in a three-arm interventional study involving adult IBS patients. We analyzed the effect of Bacillus coagulans NORDBIOTIC™ BC300, which was presented as the species with the highest efficacy in IBS patients [19], and Bifidobacterium lactis NORDBIOTIC™ BI040, the species which, when used in probiotic combinations in our earlier study in IBS-D patients, was demonstrated to improve the intensity of abdominal pain and the quality of the patients’ lives [17]. The current study has shown that both the Bifidobacterium lactis BI040 and Bacillus coagulans BC300 strains beneficially affect clinical symptoms in IBS patients but in a different range. Both strains improved the total IBS-SSS score, but Bifidobacterium lactis BI040 significantly reduced the frequency and intensity of pain, whereas Bacillus coagulans BC300 mainly ameliorated satisfaction from the bowel. Both strains beneficially affected the stool consistency, increasing the percentage of patients with normal stools as assessed with the BSF scale, but only Bifidobacterium lactis BI040 supplementation significantly decreased the number of patients with constipation in comparison with the placebo.
The obtained results, especially regarding the effect of Bacillus coagulans BC300 supplementation on IBS symptoms, are not fully consistent with the results of other researchers. Madempudi et al. showed that Bacillus coagulans Unique IS2 was efficacious in reducing abdominal pain and other IBS associated symptoms such as bloating, incomplete evacuation, urgency, bowel habit satisfaction, and stool consistency in adult IBS patients diagnosed according to the Rome III criteria (in our study, IBS patients were diagnosed according to the more restrictive Rome IV criteria) [25]. Gupta and Moity showed that Bacillus coagulans LBS improved most IBS symptoms, including the abdominal pain in an intervention group compared with the placebo group [26]. Similar results were obtained when IBS-D patients were supplemented with Bacillus coagulans MTCC 5856 [27]. Contrary to these results, our research showed that supplementation of IBS patients with Bacillus coagulans BC300 resulted in a statistically significant improvement in the global IBS symptoms as assessed by the total IBS-SSS score, but the improvement in the frequency of pain (the IBS-SSS2 score) showed only a statistically significant trend in comparison with the placebo group. The observed differences in results may be due to different ways of assessing IBS symptoms. In our study, we also used the IBS-SSS score in relation to individual symptoms. It should be emphasized that in our analysis, we assumed that an improvement occurs when there is a change in the IBS-SSS score by at least two point categories, i.e., by at least 50% compared with the baseline score. Gupta and Moity assessed the frequency of IBS symptoms with the use of the Digestive Symptom Frequency Questionnaire on a 5-point Likert scale (0 = never, 1 = ≤1 episode/week; 2 = ≤3 episodes/week; 3 = ≥3 episodes/week;
- 4 = daily episodes) [26], whereas Madenpudi et al. measured pain intensity on an 11-point numerical rating scale [25], and Maajed et al. used a 10 cm visual analog scale [27]. It should be emphasized that when stool consistency was assessed using the same BSF scale, the results did not differ. Similarly to other authors, we observed a beneficial effect of Bacillus coagulans BC300 supplementation on the normalization of stool consistency compared with the placebo group.
The current trial shows that supplementation with Bifidobacterium lactis BI040 results in a significant improvement in the clinical condition of IBS patients compared with the placebo group, mainly due to a reduction in the frequency and intensity of pain and the normalization of stool consistency. As in our study, Martoni et al. showed that Bifidobacterium lactis UABla-12 significantly reduced abdominal pain severity in IBS patients comparing with the placebo [24]. It is interesting that our earlier study of the effectiveness of combinations of probiotics containing Bifidobacterium lactis Bl040 in IBS-D patients showed
that the administration of this multi-strain probiotic, like the single strain in the current study, has a beneficial effect on pain perception [17]. Such an effect was not observed in our other study conducted according to the same protocol, in which a different combination of probiotic strains, without Bifidobacterium lactis Bl040, was used [18]. In this study, we observed a beneficial effect mainly on flatulence.
We showed that Bifidobacterium lactis Bl040, like Bacillus coagulans BC300, significantly increased the percentage of IBS patients with normal stool consistency when compared with the placebo, but only supplementation with the Bifidobacterium lactis BI040 strain decreased the number of patients with constipation, suggesting that only Bifidobacterium lactis BI040 has a beneficial effect on constipation in IBS patients. This result is in line with a recently published meta-analysis evaluating the efficacy of probiotics in patients with chronic constipation [28]. The authors demonstrated that probiotics increased stool frequency, with Bifidobacterium lactis having a significant effect, but not combinations of probiotics or single strains, such as Bacillus coagulans Unique IS2 and Lactobacillus casei Shirota.
In the current study, we have observed a strong placebo effect. Patients in the placebo group reported significant improvement of IBS symptoms as assessed by the IBS score. This effect can be explained primarily by the influence of the weekly telephone contacts, during which patients were asked in great detail about their symptoms and the effects of treatment. This is also confirmed by the observation that the beneficial effect of treatment only in the placebo group changed trend after the end of therapy. It was only after a month of followup observation that we observed most of the statistically significant differences between the intervention groups and the placebo group. On the other hand, telephone contact made it possible to control the regularity of taking the product, the weekly assessment of product tolerance, and side effects. However, we cannot rule out that the maltodextrin used as a placebo in the present study could have had a beneficial effect on patients in the placebo group. Almutairi et al., in a meta-analysis of randomized RDBPC trials, showed that orally consumed maltodextrin often (in 61.8% of analyzed trials) induced alterations in the gut microbiome, including changes in the Firmicutes and/or Bacteroidetes phyla and Lactobacillus and/or Bifidobacterium species [29]. As we assume that the intestinal microbiota plays a key role in the pathogenesis of IBS, the strong placebo effect observed in our study may be due to the direct positive effect of maltodextrin.
Strengths and Limitations of the Study
The strength of our study is that it was an RDBPC trial conducted by a team of researchers with extensive experience in this field (the researchers had conducted two other RDBPC trials evaluating the effectiveness of multi-strain probiotics in patients diagnosed with IBS-D, the results of which have been published) [17,18]. The efficiency of probiotics was assessed using IBS-SSS scores, the BSF scale, and Likert’s scales, and the safety of the probiotics was monitored during the 12-week intervention. The current study is unique in that it is one of the few studies that simultaneously evaluates the effect of two different single-strain probiotics in a three-arm intervention study, which allows for comparing effects in the same population of subjects.
Despite the numerous strengths of the study, the authors are aware of the presence of certain limitations, which include the lack of assessment of the intervention on the composition of the intestinal microbiome, which could explain the impact of both probiotic strains and maltodextrin on the gut microbiota of IBS patients. One limitation is undoubtedly the lack of assessment of the impact of the intervention on the degree of stress and anxiety associated with treatment, which could explain the strong placebo effect.
5. Conclusions
The current three-arm RDBPC interventional trial shows that both Bifidobacterium lactis NORDBIOTIC™ Bl040 and Bacillus coagulans NORDBIOTIC™ BC300 are safe and well tolerated by IBS patients and effectively improve global IBS symptoms as assessed by the IBS-SSS score, but that they have a different range of effects. Supplementation
with Bifidobacterium lactis BI040 significantly reduced the frequency and intensity of pain compared with the placebo group, while Bacillus coagulans BC300 ameliorated the satisfaction from the bowel. Both strains had a positive effect on stool consistency. The results show species/strain-specific effectiveness in IBS patients and underline the role of proper selection of probiotics for the best approach according to patients’ specific needs.
Author Contributions: Conceptualization, B.C.; methodology, B.C. and B.S.-R.; software, J.B.B. and S.A.; validation, B.C., B.S.-R., B.P.-K., H.C.-L., J.B.B. and S.A.; formal analysis, B.C., B.S.-R. and J.B.B.; investigation, B.S.-R., B.P.-K., H.C.-L., A.K.-M. and K.L.; data curation, J.B.B., S.A. and E.M.; writing—original draft preparation, B.S.-R. and B.C.; writing—review and editing, B.C., B.S.-R. and J.B.B.; visualization, B.C. and J.B.B.; supervision, B.C.; project administration, B.C.; funding acquisition, B.C. All authors have read and agreed to the published version of the manuscript.
Funding: This research was financed by Nordic Biotic Sp z o.o., Poland (grant number CT/NB/120/2020/PR-SS). Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee at the Regional Medical Chamber in Lublin (decision number 173/202l/KB/VIII).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study. Data Availability Statement: The description of the protocol study is available at https://clinicaltrials.gov “URL (accessed on 21 July 2023)” under the number NCT05064930. The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy protection.
Conflicts of Interest: B.S.-R. has served as a speaker for Polpharma, Krka, Takeda, Bayer, Promed and Alfasigma. B.C. has conducted research financed by Danone, Biomed S.A., and has conducted lectures sponsored by Nutricia, Danone, Mead Johnson, Bayer, Aurovitas, Polpharma, and Biomed S.A., B.S.-R. and B.P.-K. are members of the scientific committee of Nordic Biotic Sp. z o.o., and B.C. is a scientific chief. Other authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of the data; in the writing of the manuscript; or in the decision to publish the results.
Figures
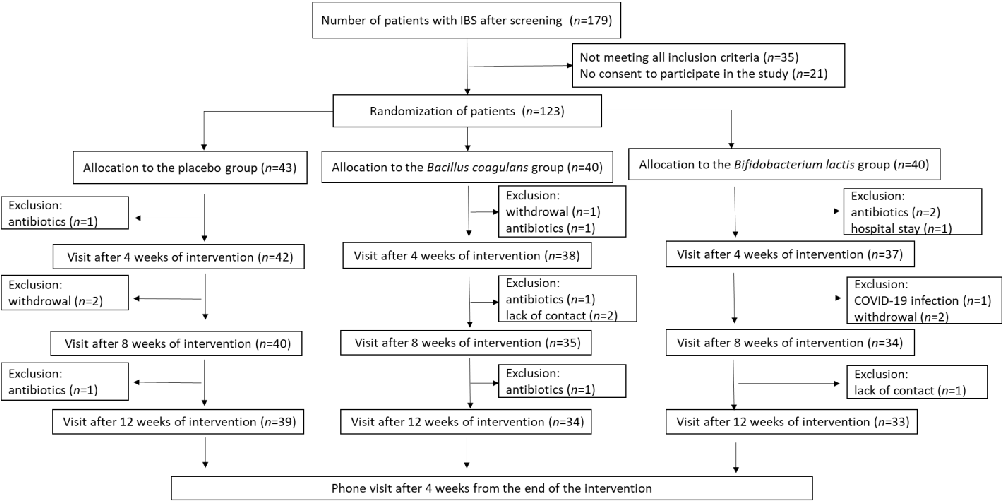
Figure 6
Supplementary outcome data from the randomized trial evaluating single-strain probiotics for irritable bowel syndrome, comparing gastrointestinal symptom improvements across treatment arms.
chart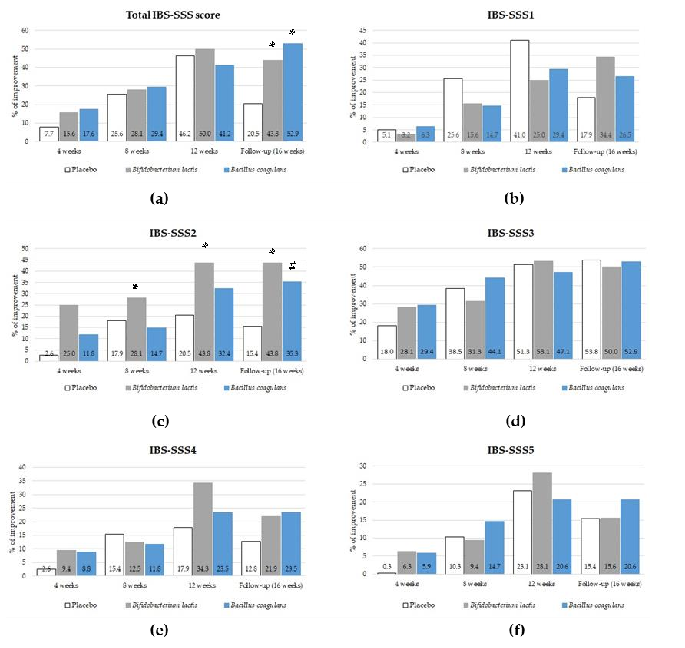
Figure 7
Probiotic intervention outcomes assessed by IBS Severity Scoring System (IBS-SSS) in a three-arm clinical trial. Both Bifidobacterium lactis BI040 and Bacillus coagulans BC300 groups showed statistically significant improvement in total IBS-SSS scores compared to placebo.
chart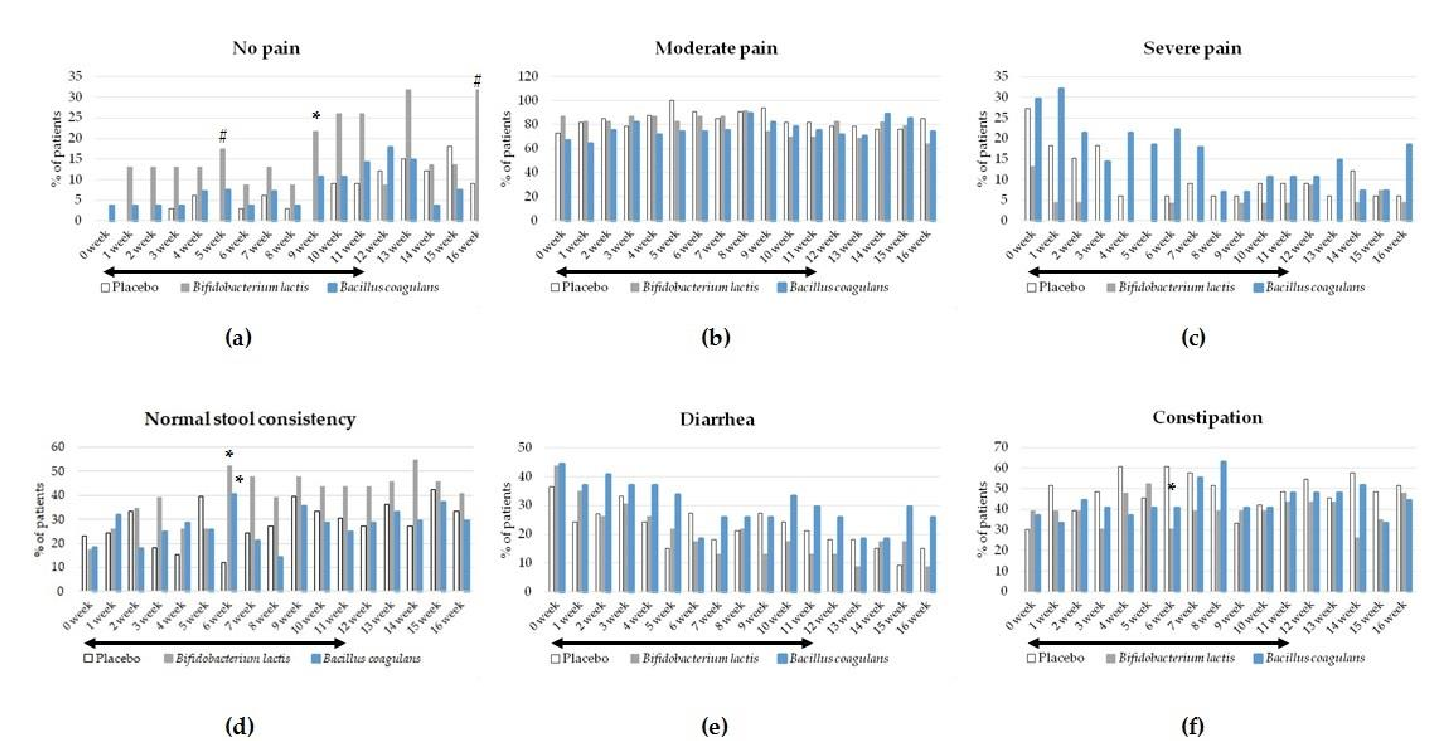
Figure 8
Supplementary outcome data from the randomized trial evaluating single-strain probiotics for irritable bowel syndrome, comparing gastrointestinal symptom improvements across treatment arms.
chart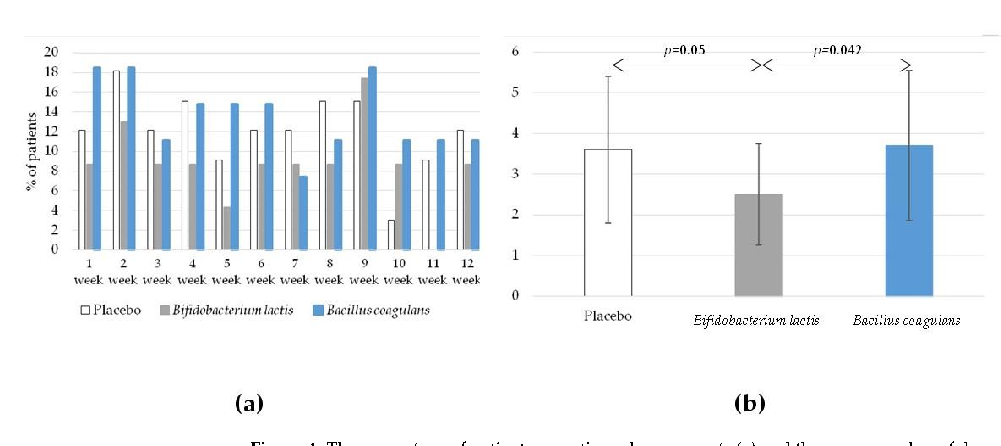
Figure 9
Supplementary outcome data from the randomized trial evaluating single-strain probiotics for irritable bowel syndrome, comparing gastrointestinal symptom improvements across treatment arms.
chartUsed In Evidence Reviews
Similar Papers
Alimentary pharmacology & therapeutics · 2009
Clinical trial: the effects of a fermented milk product containing Bifidobacterium lactis DN-173 010 on abdominal distension and gastrointestinal transit in irritable bowel syndrome with constipation.
The American journal of clinical nutrition · 2014
The effect of probiotics on functional constipation in adults: a systematic review and meta-analysis of randomized controlled trials.
World journal of gastroenterology · 2010
Systematic review of randomised controlled trials: probiotics for functional constipation.
Scandinavian journal of gastroenterology · 2011
Dose-response effect of Bifidobacterium lactis HN019 on whole gut transit time and functional gastrointestinal symptoms in adults.
World journal of gastroenterology · 2008
Effect of a fermented milk containing Bifidobacterium lactis DN-173010 on Chinese constipated women.
Journal of clinical gastroenterology · 2011